Perimenopause Starts Earlier Than You Think: Here Are the Signs at 35
Perimenopause can begin as early as age 35 — research shows more than half of women aged 30–35 experience moderate to severe perimenopause-related symptoms, often years before they receive any explanation. The earliest signs are typically sleep disruptions (especially waking between 2–4 a.m.), anxiety with no clear trigger, cycle irregularities, luteal phase mood changes, brain fog, and unexplained weight gain around the abdomen. Standard blood tests frequently miss early perimenopause because they’re designed to confirm menopause after the fact, not detect the hormonal fluctuations — particularly declining progesterone — that define the early transition.
You’re 35. You’re eating well, you’re exercising, you’re doing everything “right.” And yet something feels completely off.
You’re not sleeping the way you used to. Your moods are harder to manage. Your cycles are subtly shifting. Your anxiety has a new edge to it that wasn’t there before. And no matter what you do, the weight around your midsection won’t budge.
When you bring it up at your annual checkup, you’re told your labs look fine. You’re told you’re too young for hormones to be the issue.
But here’s the thing your doctor may not have mentioned: perimenopause doesn’t start in your late 40s. For many women, the hormonal shifts begin quietly and significantly in their mid-to-late 30s. And the symptoms get dismissed for years before anyone connects the dots.
The Timeline Nobody Told You About
This isn’t rare. This is happening quietly to a huge percentage of women in their 30s. And most of them have no idea.
Why Standard Labs Miss It
Here’s one of the most frustrating parts of early perimenopause: your standard bloodwork will often look completely normal.
A routine panel checks estradiol and FSH at one point in time. But the hormonal landscape in early perimenopause is characterized by fluctuation not simply decline. Estrogen can swing wildly high and then crash. FSH starts creeping up in response. Progesterone which is the first hormone to actually decline often isn’t even included on a standard panel.
This is why so many women in their 30s are told “everything looks fine” while feeling anything but.
The issue is that conventional testing wasn’t designed to catch perimenopause in progress. It was designed to confirm menopause after the fact.

The Signs That Show Up First
Perimenopause rarely announces itself with hot flashes and night sweats at 36. It tends to show up in quieter, more confusing ways:
Cycle changes: Your period may start coming slightly earlier or later. Cycles that were always 28 days might now be 24 or 31. Flow may become heavier or lighter. These shifts often happen years before anything dramatic.
Sleep disruptions: Waking at 2 or 3 a.m. and being unable to fall back asleep is one of the earliest and most common complaints. Progesterone has a calming, sleep-supportive effect — as it declines, sleep quality often goes first.
Anxiety with no clear trigger: Progesterone acts on GABA receptors in the brain (the same receptors targeted by anti-anxiety medications). When it drops, the nervous system loses a key regulator. This often shows up as free-floating anxiety, racing thoughts, or an inability to wind down.
Mood changes in the luteal phase: If you’ve started to dread the week or two before your period- irritability, rage, weepiness, or feeling like a completely different person — this is a hormonal signal worth taking seriously.
Brain fog and word retrieval issues: Estrogen and progesterone both influence neurotransmitter function. As they fluctuate, cognitive changes are extremely common, though rarely discussed.
Lower libido: Not just a decrease in interest, but also physical changes: vaginal dryness, less sensitivity, longer arousal time. These changes happen on a spectrum and often begin subtly.
Weight changes despite no lifestyle changes: Particularly around the abdomen. As progesterone drops and estrogen fluctuates, metabolism and fat distribution shift.
Temperature regulation issues: Not full-blown hot flashes, but feeling flushed after meals, overheating at night, or running warmer than usual.
If several of these feel familiar, your hormones — not stress, not age, not your imagination — may be the root cause.
What a DUTCH Test Actually Shows You
This is where functional testing changes everything.
The DUTCH (Dried Urine Test for Comprehensive Hormones), developed by Precision Analytical, is the gold standard for evaluating not just how much hormone you have, but how your body is using and metabolizing it.
Unlike a single serum (blood) draw, the DUTCH test:
- Measures all three forms of estrogen — estrone (E1), estradiol (E2), and estriol (E3)
- Evaluates estrogen metabolite ratios — specifically whether your body is breaking estrogen down through safer pathways (2-OH) or more inflammatory ones (4-OH and 16-OH)
- Assesses progesterone metabolites — a more complete picture than serum progesterone alone
- Maps your cortisol awakening response and diurnal pattern
- Measures DHEA-S and testosterone metabolites
- Captures melatonin — explaining sleep disruptions that standard labs miss entirely
A Real-World Example: Sarah’s DUTCH Test Results
The following is a composite case study based on clinical patterns commonly seen in women in early perimenopause. Individual results vary. This is intended for educational purposes only.
Sarah, 37. Miami. Works in marketing. Two kids, ages 5 and 8.
Sarah came in reporting: waking between 2–4 a.m. every night, heightened anxiety in the two weeks before her period, heavier periods than before, a 10-pound weight gain over 18 months she couldn’t explain, and what she described as “rage I’ve never felt before.” Her OB had run a standard panel six months prior. Everything was “normal.”
We ordered a DUTCH Complete test.
Sarah’s Initial DUTCH Results
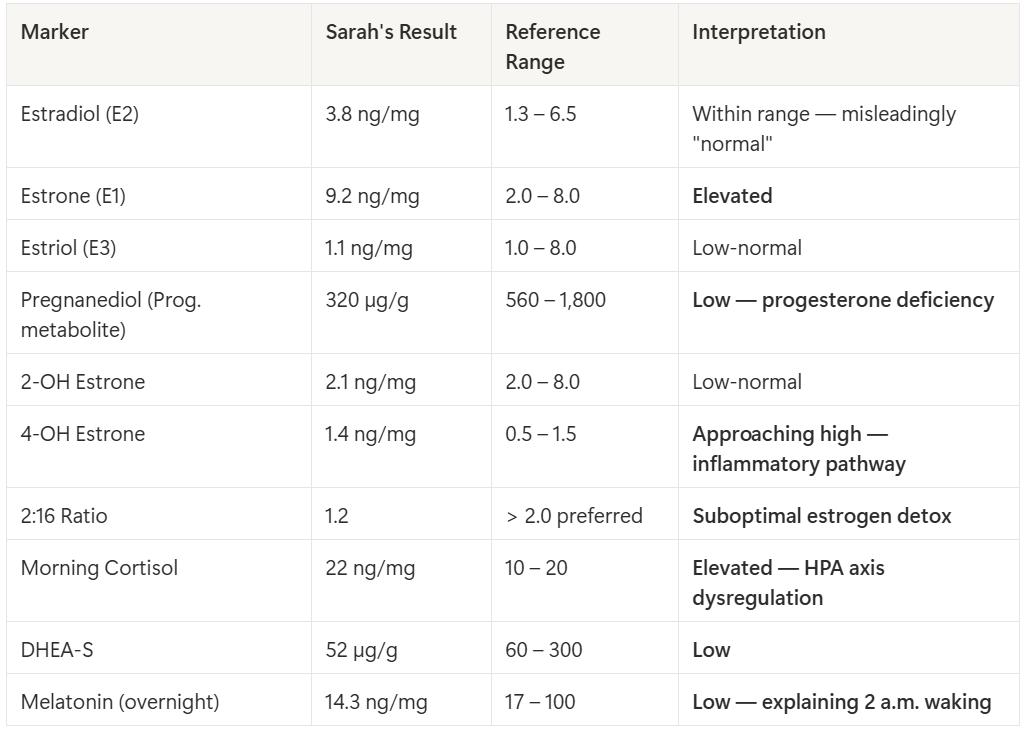
Sarah’s 90-Day Protocol
Diet: Cruciferous vegetables daily for DIM, ground flaxseed (2 tbsp), eliminated alcohol for 60 days, protein + fat at every meal, fermented foods daily.
Targeted nutrients: Magnesium glycinate (400 mg nightly), B6 as P5P (50 mg), DIM supplement (200 mg), Ashwagandha KSM-66 (300 mg twice daily), Melatonin 0.5 mg low-dose.
Lifestyle: Evening wind-down protocol, cortisol-aware exercise (strength 3x/week + daily walking), stress boundary work.
Sarah’s Follow-Up DUTCH Results (90 Days Later)
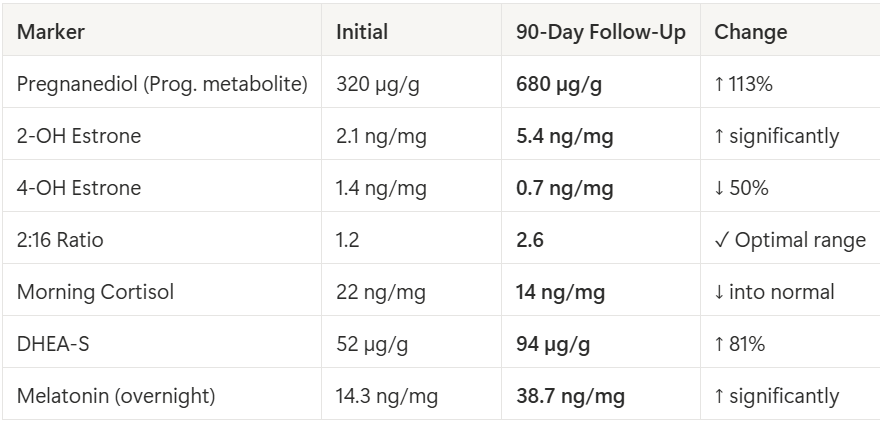
Sarah’s reported outcomes at 90 days: Sleeping through the night, luteal phase mood dramatically improved, 6 lbs released without calorie restriction, anxiety reduced ~70%, mental clarity improved, cycle stabilized at 27–28 days.
What You Can Do Right Now
- Track your cycle and symptoms across your full cycle: more informative than any single lab draw
- Reduce xenoestrogen exposure: glass containers, fragrance-free products, organic Dirty Dozen
- Eat to support estrogen metabolism : cruciferous vegetables, ground flaxseed, fiber, fermented foods
- Support your cortisol: sleep, nervous system regulation, intentional recovery
- Consider functional testing : a DUTCH Complete gives you a roadmap standard labs can’t
Want a complete gut-healing plan tailored to your symptoms, labs, and lifestyle? Book a free 15-min discovery call a free consultation with Next Generation Nutrition.
________________________
Research Referenced
Prior JC. (2020). Progesterone and ovulation across stages of the transition to menopause. PMC2783957
Ertl DA, et al. (2022). Steroid Hormone Secretion — Swiss Perimenopause Study. PMC8712488
Precision Analytical. Supporting Perimenopause with the DUTCH Test. dutchtest.com
UVA Health. (2023). Women Suffer Menopause Symptoms Decades Early. news.virginia.edu
__________________________
Written by Jessica Mantell, CNS, LDN, MS.Ed
Certified Nutrition Specialist focused on gut health, hormones, and autoimmune conditions.








